Aqualyx treatment is an injectable lipolysis service used in some aesthetic clinics for localized contouring, not for general weight loss. For licensed providers, the main question is not only whether it may fit a patient request. It is whether the clinic can deliver the service with clear eligibility criteria, consent language, training records, adverse-event planning, and traceable product sourcing.
This article keeps the focus on clinic operations. It explains where the treatment may sit within non-surgical body contouring, how to handle common patient questions, and which controls help reduce avoidable risk. Local regulatory status, scope-of-practice rules, and manufacturer instructions should always guide final protocols.
Key Takeaways
- Define the indication: Frame treatment as localized contouring, not obesity care.
- Control expectations: Use consistent language for swelling, bruising, and outcome limits.
- Document carefully: Record consent, mapping, photos, lot details, and follow-up.
- Separate protocols: Do not blend workflows across different injectable products.
- Verify sourcing: Use traceable supply channels and maintain receiving records.
Where Aqualyx Treatment Fits in Body Contouring
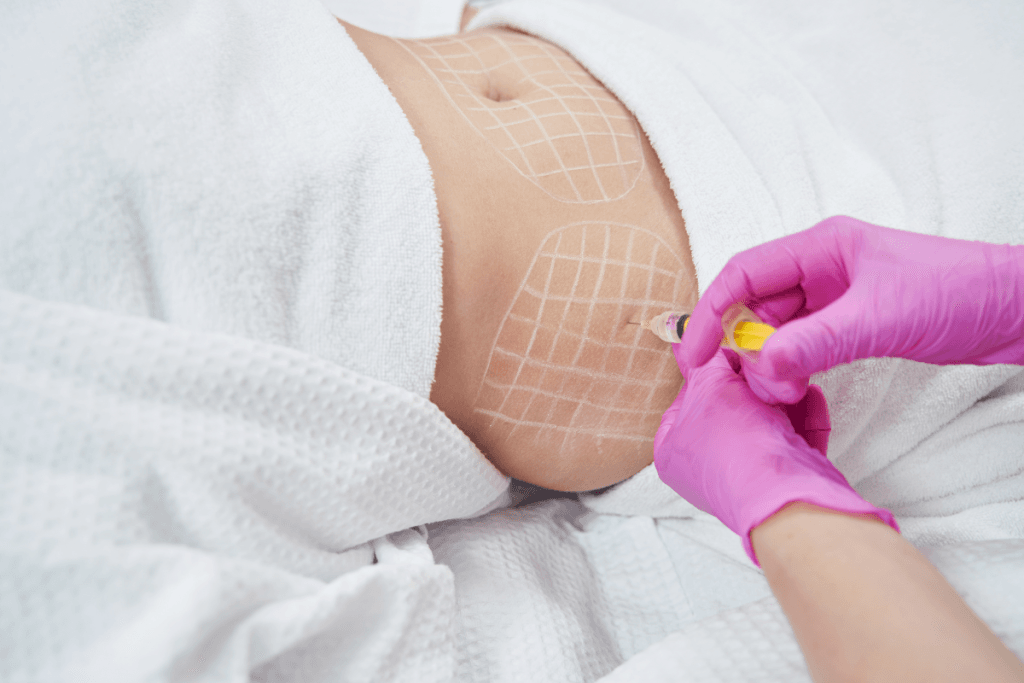
Aqualyx treatment is generally discussed as an injectable adipocytolysis option, meaning it is intended to disrupt localized adipose tissue (fat tissue) rather than manage whole-body weight. This distinction matters during consultation, marketing review, and charting. Patients may arrive with consumer phrases such as “fat dissolving,” “stubborn fat,” or “before and after,” but the clinic record should use precise, defensible language.
For service design, start by defining what your clinic will and will not treat. Many practices limit injectable contouring to small, clearly mapped areas and refer patients when surgery, medical weight management, or another pathway is more appropriate. A useful internal baseline is a short clinical summary that links patient selection, product status, and governance. For more background, see Aqualyx Clinical Overview.
Demand often comes from photo-led expectations. That can create pressure to overpromise. Clinics should avoid language that implies guaranteed fat loss, permanent results, or equivalence to liposuction. Instead, explain that visible change can vary, swelling can distort early appearance, and assessment requires consistent follow-up documentation.
Operationally, keep localized contouring separate from obesity pharmacotherapy. GLP-1 medicines and related weight-management services address metabolic and weight-reduction pathways. They are not spot-reduction treatments. If your practice offers both service lines, use different eligibility screens, consent forms, outcome measures, and follow-up schedules. The Body Contouring category can help teams separate contouring education from broader clinical topics.
Patient Selection, Consent, and Expectation Setting
Appropriate selection starts with a structured consultation, not a promise of a visible result. Your team should confirm the patient’s goals, relevant medical history, treatment area, skin quality, and tolerance for post-procedure swelling or bruising. The consult should also identify when the request falls outside the clinic’s protocol.
Consent should cover the nature of injectable lipolysis, expected local reactions, uncertainty in response, and the need for follow-up assessment. Use plain language alongside clinical terms. For example, describe edema as swelling and ecchymosis as bruising. If you mention panniculitis, define it as inflammation of subcutaneous fat.
Why it matters: Most service disputes begin with unclear expectations or incomplete records.
Many patient questions cluster around whether the treatment “works.” A clinic-safe answer is that outcomes may vary and should be assessed with standardized photography, measurements where appropriate, and clinical review. Public before-and-after images are not reliable proof. Lighting, posture, camera distance, and timing after injection can change perceived contour.
Cost questions also need careful handling. Clinics may discuss their own fee structure where allowed, but editorial and training materials should not imply standard pricing across regions or providers. Pricing can depend on consultation requirements, treatment area, product use, professional fees, and follow-up policies. Keep any public-facing materials aligned with local rules and avoid price-led clinical decision-making.
Training and Procedure Planning
Procedure planning should translate product-specific training into a controlled clinic workflow. Searches for “how to inject” or “dosage” often reflect a training gap. They should not drive clinical practice. Injectable contouring requires anatomical knowledge, aseptic technique, emergency readiness, and documented competency.
Competency records
Define who can consult, prepare, assist, inject, and triage. Your record should show the training source, date, scope, supervised practice if applicable, and any product-specific updates. If the manufacturer or an authorized trainer provides materials, store the current version in a controlled location. Retire outdated documents so staff do not rely on conflicting instructions.
Training should cover more than injection technique. Include patient communication, photography standards, sterile preparation, waste handling, documentation, and escalation. A practical setup resource is Aqualyx Injections Procedure, which can support internal checklist development when adapted to local governance.
Treatment mapping
Mapping is both a clinical and documentation control. The chart should show the treated area, planned entry sites, relevant landmarks, and what was actually performed. Use standard body diagrams and repeatable photo angles. This becomes especially important when different clinicians review follow-up visits or when patients compare images from social media.
Questions such as “how much per area” or “how many vials” should not be answered with a generic number in a clinic policy. Volumes, spacing, and treatment planning depend on anatomy, product guidance, clinician training, and local rules. Your protocol can state that dosing and delivery parameters must follow current manufacturer instructions and documented training, with any deviations justified in the chart.
Quick tip: Keep one controlled protocol version in your quality system.
Safety Planning: Expected Reactions and Red Flags
Safety planning should distinguish common local reactions from symptoms that require prompt escalation. Swelling, tenderness, bruising, firmness, and redness may drive most routine follow-up calls. Staff need scripts that explain what was discussed at consent, what information to collect, and when a clinician must review the case.
Online searches for side effects, long-term concerns, or “gone wrong” outcomes often mix expected inflammation with uncommon complications. Clinics should respond with neutral triage, not reassurance that skips assessment. Record onset, location, severity, photos when appropriate, patient contact attempts, advice provided, and final disposition.
Escalation policies should be written before the first appointment. Include pathways for suspected infection, severe or worsening pain, skin color change, ulceration, systemic symptoms, allergic-type reactions, or any presentation outside the expected recovery pattern. Staff who receive messages or photos after hours need clear authority limits and a route to a responsible clinician.
Patients may also ask about liver effects or systemic risk. Keep those discussions evidence-based and conservative. Risk assessment should sit within the medical history process, including relevant comorbidities, medicines, allergies, pregnancy status where applicable, and prior aesthetic procedures. If risk is uncertain, defer to the medical director’s policy and local standards.
Evidence Signals: Photos, Reviews, and Outcome Records
Before-and-after content can help with internal audit only when capture conditions are controlled. Public images rarely meet that standard. A clinic should use the same background, lighting, camera distance, body position, and timing across visits. Otherwise, normal variation can look like treatment response or treatment failure.
Outcome records should include dates, treatment area, relevant measurements if used, photo set, reported symptoms, and concurrent procedures. Note confounders such as recent illness, major weight change, fluid shifts, or other contouring services. These details help clinicians interpret results without relying on memory or subjective impressions.
Patient reviews can still provide service insight. Separate operational feedback, such as scheduling and follow-up communication, from clinical concerns, such as unexpected swelling or dissatisfaction with appearance. This distinction helps practice managers improve workflow while preserving clinical review for medical issues.
When using educational images, confirm consent, provenance, and context. Avoid showing severe reaction photos without clinical framing. Some images circulating online are mislabeled, edited, or unrelated to the product named in the post. For broader staff education on injectable contouring language, review Fat Dissolving Injections.
Comparing Injectable and Non-Injectable Options
Comparisons should focus on workflow fit, evidence quality, regulatory status, and follow-up burden rather than brand preference. Patients may ask whether one injectable is “better” than another, or whether treatment is like a prescription weight-loss medication. A clinic-safe response is to explain that these options serve different purposes and require different assessment pathways.
Injectable lipolysis products can differ in composition, training requirements, handling, labeling, and local regulatory status. If your clinic evaluates alternatives, keep each product in its own protocol with its own consent wording and adverse-event plan. Background reading on related injectable approaches includes Phosphatidylcholine Benefits and Alidya vs Aqualyx.
Device-based contouring may avoid injections but creates different operational demands, including device maintenance, operator training, photography standards, and patient suitability checks. Surgical options may be more appropriate for larger-volume contouring or cases outside the clinic’s non-surgical protocol. Referral criteria should be explicit and documented.
Product-level navigation can support procurement review, but it should not replace clinical governance. If your team references Aqualyx 10 x 8 mL Vials, keep that link separate from the controlled procedure protocol. MedWholesaleSupplies serves licensed clinics and healthcare professionals, with brand-name products sourced through vetted distributor and verified supply channels.
Documentation, Sourcing, and Inventory Controls
Clinic outcomes depend partly on operational reliability. Every aqualyx treatment should sit inside the same governance system used for other injectable procedure supplies. That includes procurement checks, receiving logs, storage conditions, charting standards, and incident documentation.
Use a short checklist that staff can complete consistently:
- Credential check: Confirm role, scope, and supervision.
- Consult record: Capture goals, history, consent, and photos.
- Product verification: Record supplier, lot, expiry, and package integrity.
- Protocol match: Confirm the scheduled service and product align.
- Storage review: Follow manufacturer instructions and local policy.
- Procedure notes: Chart mapping, area treated, and aftercare given.
- Follow-up log: Document outcomes, calls, photos, and escalation.
For procurement, use a two-step check where possible. Administrative staff can verify vendor documentation and receiving details. The clinical lead can confirm product labeling, protocol match, and suitability for the scheduled service. This reduces mix-ups when clinics carry multiple body-contouring products or rotate staff across rooms.
MedWholesaleSupplies operates as a B2B supplier for licensed clinics, so procurement workflows should still remain clinic-owned and auditable. Keep purchase references, item identification, and clinical protocols in distinct folders. Staff should not infer technique, dosing, or eligibility from a product page.
If your team reviews related products, apply the same separation. A product such as Phosphatidylcholine 5 Vials or Lemonbottle Ampoule Solution should have its own documentation pathway. The Clinic Operations category can support broader workflow planning across services.
Authoritative Sources
Use regulator and public-health sources to support safety governance, then apply local law, manufacturer instructions, and medical-director policy. These references do not replace product-specific training or jurisdictional requirements.
- CDC injection safety guidance
- FDA warning on unapproved fat-dissolving injections
- FDA DSCSA information for supply-chain traceability
Review these sources during policy updates, staff onboarding, and incident review. If regulations, product status, or staffing models change, update your consent forms, training records, and procurement checks before expanding the service.
This content is for informational purposes only and is not a substitute for professional medical advice.




