Facial contours change with age, weight shifts, and skin quality. In clinic, patients often describe “looking tired” or “deflated.” Facial volume restoration is the clinical lens that separates true structural loss from surface changes. That distinction helps you choose a plan, set expectations, and document outcomes.
For practice teams, volume work is also operational. Product category selection, lot tracking, informed consent, and photo standards can determine whether results look consistent across providers.
Key Takeaways
- Separate volume loss from laxity early to avoid mismatched plans.
- Map changes by zone: temples, midface, perioral, and tear troughs.
- Compare modalities by mechanism, reversibility, and follow-up burden.
- Standardize documentation, lot capture, and authenticity verification.
Facial Volume Restoration: A Practical Clinical Framework
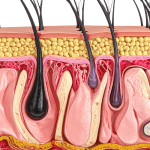
In day-to-day terms, “volume” is the three-dimensional support that keeps light reflecting off the midface and cheeks, and keeps hollows from reading as fatigue. Clinically, the drivers include fat pad remodeling, ligament laxity, dermal thinning, and skeletal change over time. Patients may experience midface flattening, temple hollowing, deeper nasolabial folds, and under-eye shadowing.
Start by anchoring the conversation in anatomy and mechanics. You can explain that the face is not one compartment. The temples, malar (cheekbone) region, deep medial cheek, and perioral area age differently. That framing reduces “one syringe fixes all” expectations and supports zone-based planning.
Why it matters: Treating laxity like volume loss can create unnatural projection.
Operationally, your framework should also define what “success” looks like. For many clinics, that means consistent pre/post photography, a documented aesthetic goal, and a shared language for describing correction by area rather than by brand.
MedWholesaleSupplies supplies only to licensed healthcare practices.
For deeper background on common filler classes and positioning, see Types Of Dermal Fillers. You can also orient new staff to your formulary by browsing the Dermal Fillers Category and your internal protocols for each class.
What Drives Volume Loss Across the Face
Face volume loss is rarely a single-process problem. Age-related facial fat loss can involve both superficial and deep fat compartments, with redistribution that changes highlights and shadows. Bone resorption (gradual bone thinning) can further reduce structural support, especially around the orbit and maxilla. Add collagen and elastin changes in the dermis, and the same face can look flatter and less “lifted” even without major weight change.
Patients sometimes report sudden loss of volume in face after an illness, stress, or weight change. In practice, you can treat “sudden” as a timing clue rather than a diagnosis. Recent weight loss, changes in training load, medication changes, and systemic conditions can all affect perceived fullness. Your intake should capture these factors and support appropriate referral when something seems out of pattern for cosmetic aging.
Zone patterns that matter for planning
Different zones signal different mechanics. Temple hollowing often reads as skeletalization and can widen the upper face. Midface volume loss tends to flatten the cheek and deepen the nasolabial crease. Tear trough hollowing can be true depression, shadowing from lid-cheek junction changes, or both. Perioral changes can blend dental support, lip volume, and skin texture. A zone map helps you avoid chasing a single line or fold.
Volume loss versus skin quality
Patients often conflate thin skin with volume loss. Dermal thinning, dyschromia, and textural changes can make shadows look deeper. That is why “skin tightening vs volume restoration” is a useful internal prompt. One improves envelope and surface. The other rebuilds support. When you label the dominant issue correctly, you can explain why a plan may involve more than one modality, staged over time, with conservative goals.
When teams align on these patterns, facial volume restoration discussions become clearer and easier to document.
Inventory is sourced as brand-name units through screened distribution channels.
Assessment: Mapping Changes and Setting Expectations
A consistent assessment reduces rework and improves patient understanding. Start with standardized photos and a quick zone-based exam. Note baseline asymmetry and prior procedures, including energy-based treatments and threads. If a patient asks how to prevent volume loss in face, your role is to frame risk factors and modifiable contributors at a high level, without promising prevention. Weight cycling, smoking, sun exposure, and general health can influence facial appearance over time.
Use structured language in the chart. Document the primary concern (“midface flattening,” “temple concavity,” “tear trough shadowing”) and the suspected driver (“loss of support,” “skin laxity,” “textural change”). That makes it easier to justify why you are discussing cheek volume restoration options rather than only treating the nasolabial fold as a line.
Clinic checklist: pre-treatment documentation
- Baseline photo set
- Prior procedures and dates
- Bleeding-risk discussion noted
- Allergy and sensitivity history
- Patient-stated outcome goals
- Planned zones and rationale
- Product class recorded
Patients also ask about “restore facial volume without fillers.” This is a good time to explain the difference between structural replacement and general skin quality support. You can outline which concerns respond to non surgical facial volume restoration approaches and which typically require true volumization.
For staff training on what different filler classes are designed to do, the Dermal Fillers Product Hub can help teams see how products are grouped by type.
Intervention Options and How to Compare Them
Most volumization plans combine more than one mechanism. Injectables can replace volume directly or stimulate collagen over time, depending on class and technique. Energy-based devices can improve skin texture and apparent tightness, but they do not replace deeper structural support. Surgical options, including fat transfer, can provide larger-volume change but have different operational requirements and consent complexity.
From a practice standpoint, comparison is less about “best treatment for loss of volume in face” in the abstract and more about fit for zone, reversibility, onset expectations, and follow-up cadence. Your patient’s risk tolerance and history of prior products also matters.
| Modality | What It Targets | Operational Notes |
|---|---|---|
| Hyaluronic acid gel fillers | Direct space-filling and contour | Often chosen when adjustability is important; document lot and reversibility discussion. |
| Biostimulatory injectables | Collagen remodeling support | Requires clear expectation-setting; track sessions and area plans carefully. |
| Calcium-based fillers | Structural support and contour | Technique-sensitive; ensure team consistency and post-care documentation. |
| Autologous fat transfer | Higher-volume restoration | Procedure and handling vary by setting; align consent and follow-up workflows. |
| Energy-based devices | Skin texture and tightening | Useful adjunct for envelope; set boundaries versus true volume replacement. |
If your team wants a tighter clinical comparison between common classes, review Calcium Hydroxylapatite Vs PLLA.
For hyaluronic acid options used in contouring, many clinics start by browsing the Hyaluronic Acid Fillers category and then narrowing by intended plane and area, per label and training.
When you do discuss specific examples, keep it high-level. Some practices reference products such as Sculptra 2 Vials when explaining collagen stimulation concepts. Others may point to Radiesse 3 mL when describing calcium hydroxylapatite as a structural class. Product selection and technique should follow training and the official labeling.
For reading that mirrors common patient comparisons, see Sculptra Vs Juvederm and Radiesse Vs Juvederm Voluma.
Adjuncts Patients Ask About (Lifestyle and Devices)
Patients frequently ask how to restore cheek volume naturally or how to restore fat pads in face naturally. It helps to be precise with language. Lifestyle changes can support overall skin and body composition, but they usually cannot recreate the anatomic projection that is lost with compartmental fat changes or skeletal remodeling. Still, these conversations matter because they affect adherence and satisfaction.
Diet and nutrition for facial volume is typically discussed as general health support. Adequate protein intake, stable weight patterns, and addressing micronutrient gaps may support skin and connective tissue maintenance. Collagen for facial volume support is a common question. You can explain that oral supplements are not equivalent to volumizing procedures, and evidence varies by outcome measured. Avoid promising changes in facial fullness.
Devices and exercises: what to say, what to avoid
“Facial volume exercises” often circulate online. You can acknowledge that facial movement can affect tone and awareness, but it does not selectively rebuild deep fat compartments. For radiofrequency microneedling for volume, frame it as primarily improving texture and perceived tightness. If patients equate tightening with filling, restate the distinction between envelope improvement and true volumization. This keeps expectations aligned and reduces dissatisfaction when hollows persist.
Hormones and facial fat distribution also comes up, especially around menopause, androgen changes, or thyroid disease. A neutral approach is best. You can document the concern and suggest medical evaluation for systemic symptoms, while keeping your aesthetic plan within scope.
When these adjuncts are discussed in the context of facial volume restoration, the key is clear boundaries and careful charting.
Practice Operations and Procurement Considerations
Volume-focused services have predictable operational pressure points: authenticity verification, traceability, and consistent storage practices. Even when clinical technique is strong, inconsistent documentation can create avoidable risk during audits or adverse-event follow-up. Policies vary by jurisdiction, but most clinics benefit from a repeatable workflow that ties product receipt to patient administration records.
Quick tip: Build a standardized lot-number capture step into your chart template.
Clinic workflow snapshot
- Verify licensure eligibility
- Confirm formulary and indications
- Receive and inspect shipment
- Record lot and expiry
- Store per labeling
- Document administration details
- Maintain traceability records
MedWholesaleSupplies focuses on authentic, brand-name medical products for professional use. That matters when you are reconciling lot numbers, expiration dates, and supplier documentation across multiple providers.
Also consider how you educate new staff on what each product is for, without turning education into brand preference. If you reference examples in onboarding, keep it neutral and evidence-based. Some teams use a single-page explainer alongside a link to a background article such as Sculptra Aesthetic Overview to explain the idea of collagen stimulation versus immediate gel fill. If you include a hyaluronic acid example in your training set, ensure everyone knows where labeling, anatomy training, and complication protocols are stored.
MedWholesaleSupplies sources products through vetted distributor relationships.
Authoritative Sources
When you need patient-facing risk language, contraindication details, or adverse-event reporting pathways, rely on primary sources. Your counseling and consent should align with the product’s official labeling and your governing body’s standards. For injectables, it is also useful to maintain a clinic library of complication management protocols, including vascular occlusion recognition and escalation steps, based on published guidance and training.
The following references can support internal training and policy writing. They are not a substitute for product labeling or hands-on education.
- Neutral overview of dermal filler risks and regulation: FDA soft tissue fillers (dermal fillers)
- Professional society background on dermal filler use: American Society of Plastic Surgeons dermal fillers
- Dermatology perspective on cosmetic injectables: American Academy of Dermatology on fillers
Further reading can be most useful when it’s role-based. Consider a short packet for front desk (photo standards and scheduling), nursing (post-procedure instructions templates), and clinicians (anatomy, product classes, and complication pathways). Keep updates version-controlled so your whole team stays aligned.
This content is for informational purposes only and is not a substitute for professional medical advice.