
The two layers of the dermis are the papillary dermis and the reticular dermis. The papillary dermis is the thin, superficial layer just below the epidermis. The reticular dermis is the thicker, deeper layer above the hypodermis, or subcutaneous tissue. Clinically, what are the two layers of the dermis matters because layer depth can affect bleeding, sensation, edema, tissue handling, and documentation language during skin procedures.
Key Takeaways
- Two-layer model: The papillary dermis is superficial; the reticular dermis is deeper and thicker.
- Clinical relevance: Dermal depth influences vascular response, sensory feedback, and product placement language.
- Boundary awareness: The dermis blends into the hypodermis, with thickness varying by site, age, and body habitus.
- Documentation value: Record intended tissue plane, anatomic site, device, lot, and UDI where applicable.
- Training focus: Pair anatomy terms with plain-language depth descriptions to reduce staff ambiguity.
Where the Dermis Sits in Skin Anatomy
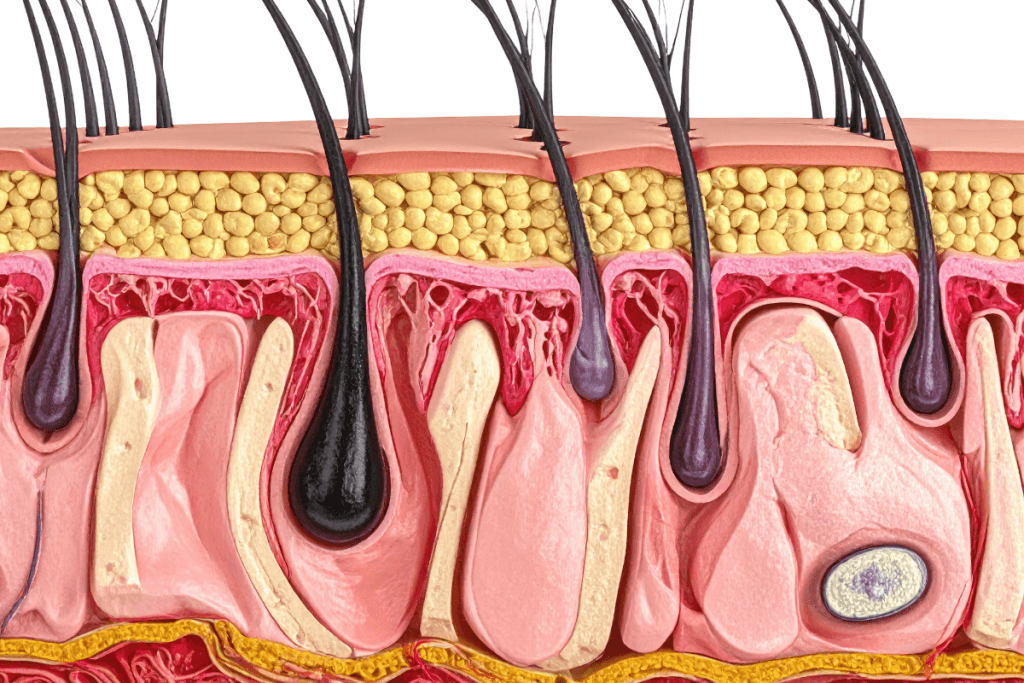
The dermis sits between the epidermis and the hypodermis. The epidermis is the outer barrier layer and is avascular, meaning it lacks blood vessels. The dermis is vascular, innervated, and made of connective tissue that supports skin strength, elasticity, immune response, and repair.
For a fuller review of the outer skin layer, see Layers Of The Epidermis. The epidermis has named strata, while the dermis is usually described by its two connective-tissue zones. These zones are continuous rather than cleanly separated under the microscope.
Clinicians often ask what are the two layers of the dermis when they are translating anatomy into real procedural language. In charting, “superficial dermal” usually maps to the papillary dermis. “Deep dermal” usually maps to the reticular dermis. “Subcutaneous” usually refers to the hypodermis, although the dermis-hypodermis interface can be irregular.
Why it matters: A few millimeters can change tissue response, especially in thin skin or high-mobility sites.
Papillary Dermis: The Superficial Layer
The papillary dermis is the upper dermal layer, positioned immediately below the epidermis. It interlocks with the epidermis through dermal papillae, which are small projections that increase contact between the two layers. This arrangement supports nutrient diffusion to the avascular epidermis and strengthens the dermal-epidermal junction.
Histologically, the papillary layer is often described as loose areolar connective tissue. That means its collagen fibers are finer and less densely packed than those in the deeper dermis. It also contains capillary loops, lymphatic channels, sensory nerve endings, fibroblasts, immune cells, and extracellular matrix, the supportive gel-like scaffold around cells.
The papillary dermis helps with thermoregulation, immune surveillance, light-touch sensation, and early wound response. In clinical observation, this is the layer most closely associated with visible erythema, superficial wheal formation, and fine capillary bleeding. It is also the layer clinicians often mean when they use the term “intradermal,” although exact usage varies by specialty and technique.
When teams document superficial dermal work, the term should not stand alone. Add a brief anatomic descriptor, such as “superficial dermis near the dermal-epidermal junction,” when that level of detail helps quality review or training.
Reticular Dermis: The Deeper Support Layer
The reticular dermis is the deeper and thicker dermal layer. It sits below the papillary dermis and above the hypodermis. Compared with the papillary layer, it has denser collagen bundles and more organized elastic fibers, which contribute to tensile strength and skin resilience.
This layer is commonly described as dense irregular connective tissue. “Dense” reflects its collagen-rich structure. “Irregular” means the fibers run in multiple directions, allowing the skin to tolerate stress from more than one angle. The reticular dermis also contains larger blood vessels, lymphatics, nerve fibers, fibroblasts, and portions of skin appendages, depending on body site.
Hair follicles, sebaceous glands, and sweat glands may extend into or through this region. The deeper vascular plexus helps with thermoregulation and inflammatory response. From a procedural standpoint, deeper dermal involvement may change the degree of discomfort, bruising risk, diffusion pattern, and tissue resistance felt during needle or cannula movement.
That does not mean the reticular dermis has one uniform clinical feel. Skin thickness varies substantially across the face, trunk, extremities, palms, soles, and chronically sun-exposed areas. Age-related collagen change and prior procedures can also alter tissue texture.
What the Dermis Contains and Why Clinics Care
The dermis contains collagen, elastin, fibroblasts, immune cells, blood vessels, lymphatic channels, nerve endings, and site-dependent appendages. These structures explain why dermal procedures can produce bleeding, edema, tenderness, erythema, or altered sensation even when the epidermis appears only minimally disrupted.
Collagen provides tensile strength. Elastin supports recoil. Fibroblasts produce and remodel extracellular matrix. Nerve endings transmit pain, pressure, temperature, and touch. Vessels support thermoregulation and wound healing but also create a route for bruising after tissue trauma.
For a deeper companion discussion, see Two Layers Of The Dermis. Teams that train across dermatology, aesthetics, wound care, or device-based services benefit from using the same vocabulary for these structures.
Plain-language mapping helps during onboarding. “Upper dermis” can refer to the papillary layer. “Lower dermis” can refer to the reticular layer. “Fat layer” usually refers to the hypodermis. These plain terms should support, not replace, the clinical terms used in procedure notes.
Dermis, Epidermis, and Hypodermis: Avoiding Common Confusion
The skin is often described as having three main layers: epidermis, dermis, and hypodermis. Within those broad layers, the epidermis has multiple strata, while the dermis has two main layers. This is why learners may see both “three layers of skin” and “two layers of the dermis” in anatomy materials.
The epidermis provides barrier function and continual cellular renewal. The dermis provides mechanical support, vascular supply, sensation, thermoregulation, and wound repair capacity. The hypodermis, also called subcutaneous tissue, contains adipose lobules, connective tissue septa, larger vessels, and larger nerves.
For sequence-based epidermal review, Epidermis In Order explains how epidermal strata progress from basal cell renewal to surface barrier. For barrier function context, Function Of The Epidermis connects epidermal structure with hydration, irritation, and barrier integrity.
| Layer | Plain-language description | Typical contents | Clinical relevance |
|---|---|---|---|
| Papillary dermis | Upper dermis | Fine collagen, capillaries, sensory endings, immune cells | Visible reactivity, superficial bleeding, early inflammatory change |
| Reticular dermis | Deeper dermis | Dense collagen, elastic fibers, larger vessels, appendage support | Tensile strength, deeper sensory response, structural support |
| Hypodermis | Subcutaneous fat layer | Adipose lobules, septa, larger vessels and nerves | Variable thickness, glide plane, common injection target |
The hypodermis is not one of the two dermal layers. It sits below the dermis and serves different functions, including cushioning, insulation, energy storage, and mobility over deeper fascia. In practice, however, the boundary matters because deeper placement can shift a procedure from dermal to subcutaneous tissue.
Procedure-Relevant Depth Language
In clinical workflows, dermal anatomy is most useful when it reduces ambiguity. Staff may agree on a device or technique but still use different meanings for “intradermal,” “superficial,” “deep,” and “subcutaneous.” Standardized depth language supports training, handoffs, adverse-event review, and chart consistency.
When documenting what are the two layers of the dermis for competency materials, pair each term with a short tissue-plane description. For example, “papillary dermis” can be described as the upper dermis near the dermal-epidermal junction. “Reticular dermis” can be described as the deeper collagen-rich dermis above subcutaneous fat.
Clinical endpoints also vary by site. Thin eyelid skin, thick palmar skin, and mobile perioral skin do not behave the same way. Tissue laxity, edema, scarring, inflammation, and prior procedures can further change resistance and visible response. These factors should be considered when a clinic writes internal protocols or trains new operators.
- Define plane terms: Align superficial, deep, intradermal, and subcutaneous wording.
- Document the target: Record intended layer and anatomic site.
- Note visible response: Capture expected erythema, wheal, bleeding, or swelling when relevant.
- Track identifiers: Include device, lot, serial, or UDI when applicable.
- Match policy: Keep technique language aligned with labeling and clinic SOPs.
Quick tip: Use one diagram set across training, consent templates, and procedure notes.
Tools, Products, and Clinic Operations
Device choice often implies an intended tissue plane, so anatomy education should connect with procurement and documentation controls. A clinic that stocks tools for superficial, dermal, and subcutaneous workflows should define how each item fits approved procedures, training sign-off, and charting language.
For example, intradermal delivery devices such as Micronjet may be used in protocols that require controlled superficial placement, where appropriate to labeling and clinic policy. Fine-gauge microneedle systems such as Fillmed Nanosoft Microneedles may support shallow technique standardization in selected settings. Product selection should remain tied to indications, operator training, and local requirements.
For injectable aesthetic planning more broadly, Types Of Dermal Fillers provides a practical selection framework. That topic is distinct from basic dermis anatomy, but both require precise tissue-plane language and clear charting.
MedWholesaleSupplies serves licensed clinics and healthcare professionals, with brand-name medical products sourced through vetted distribution pathways. That role is relevant when practices connect anatomy-based procedure protocols with sourcing records, lot traceability, and internal compliance review.
Clinics building post-procedure or adjunctive skin-support protocols can also browse the Clinical Skincare collection. Treat category pages as navigation resources rather than clinical evidence. Procedure-specific decisions should still follow professional judgment, labeling, and written clinic policy.
Authoritative Sources
For standard terminology and anatomy review, the following sources provide useful reference points:
- NCBI Bookshelf review of dermis histology
- NCBI Bookshelf overview of skin anatomy
- OpenStax chapter on skin layers
In summary, what are the two layers of the dermis has a simple answer: papillary and reticular. The clinical value comes from applying those terms consistently to depth, tissue response, documentation, and product-related workflows. Use precise language, confirm technique expectations during training, and defer to labeling and clinic policy for procedure-specific decisions.
This content is for informational purposes only and is not a substitute for professional medical advice.




