Hyaluronic acid shows up across aesthetics, dermatology, and medspa-adjacent care. It can be a topical humectant (water-binding ingredient), an injectable device component, or a dietary supplement. That variety creates confusion during protocol updates, product reviews, and patient counseling. Teams also hear the same baseline question: what is hyaluronic acid, and why does it behave differently across formats?
This guide is written for licensed healthcare providers and clinic operations teams. It focuses on practical distinctions, conservative safety framing, and workflow considerations. It does not cover dosing, injection technique, or patient-specific recommendations.
Key Takeaways
- Hyaluronic acid is a water-binding glycosaminoglycan in human connective tissue.
- Topical, injectable, and oral forms differ in regulation and risk.
- Formulation details matter more than marketing terms in practice.
- Clinic documentation should support traceability and adverse event review.
what is hyaluronic acid for Aesthetic Medicine Teams?
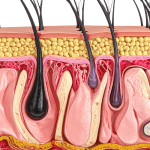
Hyaluronic acid (HA) is a naturally occurring polysaccharide found in skin, joints, and the extracellular matrix (the body’s structural “scaffold” between cells). It binds water and contributes to tissue hydration and viscoelasticity (stretch-and-recoil behavior). In aesthetic medicine, you’ll see HA discussed in three main contexts: skin hydration support, soft-tissue contouring, and barrier-friendly skincare formulations.
The same name can describe very different materials. HA can be low or high molecular weight, linear or cross-linked, and combined with other excipients. These changes influence how long it persists, how it spreads in tissue, and how it performs in a topical product versus an injectable device. That is why a “serum HA” is not operationally comparable to an “injectable HA,” even if both aim to improve skin hydration.
A quick structure-and-function refresher
HA is made of repeating sugar units and can hold water within its molecular network. In skin, it is one contributor to softness and pliability, alongside collagen, elastin, and lipids. In products, HA is often present as sodium hyaluronate (a salt form used for stability). In injectables, HA may be modified (for example, cross-linking) to alter how it behaves after placement. These are high-level concepts only; product-specific properties should be confirmed using the manufacturer’s instructions for use and published technical documentation.
When teams ask “what is hyaluronic acid made from,” the answer is usually process-based. Modern medical and cosmetic HA is commonly produced via microbial fermentation, then purified. Some sources may be animal-derived, depending on the manufacturer and product line. For clinics, the key is not the origin story alone. The key is traceability, documentation, and fit with your clinical governance.
Trust cue: Many suppliers limit purchasing access to licensed healthcare accounts.
Where HA Fits in Aesthetic Services and Product Mix
In aesthetics, HA may be used as a topical ingredient for hydration, as an injectable dermal filler material, or within “skin booster” style devices intended to support dermal hydration and skin quality. Your clinic’s use cases determine which standards matter most: ingredient review for topicals, device traceability for injectables, or supplement quality review for oral products.
From a sourcing perspective, it helps to start with the category rather than the brand. For example, procurement teams often browse Dermal Fillers broadly, then narrow to Hyaluronic Acid Dermal Fillers when standardizing training, storage, and documentation steps. For clinical education, deeper background can be useful, such as Hyaluronic Acid vs Non Hyaluronic Acid Fillers and Skin Boosters Injections.
Why it matters: “Hydration” and “volume” goals can imply different products, risks, and documentation needs.
Operational differences by format
The question what is hyaluronic acid becomes operationally relevant when you map format to governance. Topical products typically fall under cosmetics rules, and your main tasks are ingredient review, patient tolerance screening, and consistent retail documentation policies (if applicable). Injectable HA devices may require heightened controls: receiving checks, lot and expiry tracking, temperature requirements per IFU, and adverse event reporting pathways. Oral supplements add a different set of controls, including label review, supplier qualification, and a clear “not a drug” counseling boundary.
| Format | Primary use in aesthetics | What clinics should verify | Common limits |
|---|---|---|---|
| Topical HA (serums/creams) | Surface hydration, comfort, barrier support | Ingredient list, patient tolerability, compatible routines | Short wear time; depends on occlusive layering |
| Injectable HA devices | Soft-tissue contouring or dermal hydration devices | IFU, indications, storage, lot traceability, training requirements | Procedure risks; outcomes depend on technique and selection |
| Oral HA supplements | Adjunct “skin and joint” wellness positioning | Label claims, quality documentation, contraindication screening process | Variable evidence; patient expectations often exceed data |
Some clinics keep exemplar SKUs available for staff education and packaging review, without turning education into promotion. Examples of site-listed products that fall into HA-adjacent aesthetic workflows include Profhilo HL Prefilled Syringe and Restylane Skinboosters Vital. When you reference any device publicly or in protocols, align language to the IFU and local regulations.
Topical HA in Skincare Protocols: Serums, “Glow,” and Oily Skin
Most clinicians encounter HA first as a topical humectant. A hyaluronic acid serum is typically designed to increase water content in the stratum corneum (the outer skin layer). That can reduce tightness and improve the look of dryness lines. It also supports comfort after procedures that temporarily compromise barrier function, when used appropriately and with clinician oversight.
Formulation details drive real-world results. HA can sit at different molecular weights and may be blended with glycerin, panthenol, ceramides, or light occlusives. Patients often apply serums on dry skin, which can feel tight later. A better general approach is applying to slightly damp skin and sealing with a moisturizer if tolerated. This is not a prescription instruction. It is a workflow talking point for staff education and consistent messaging.
Addressing common “fit” questions in consults
Clinics frequently hear, “is hyaluronic acid good for oily skin?” Often it can be, because humectants are not inherently comedogenic (pore-clogging). The risk is less about HA itself and more about the vehicle, added oils, fragrances, and layering habits. Another common question is whether it is good for young skin. In practice, HA is not “age-specific.” It is more about barrier status, irritation patterns, and what else is in the routine. If patients are acne-prone, consider a simple, fragrance-minimized formulation and clear stop rules for irritation.
For teams wanting additional context, see Multiple Health and Cosmetic Benefits for a general overview. Keep claims conservative in your own materials. “Hydration support” is easier to substantiate than “rebuilding” or “tightening” language.
Oral HA Supplements: Evidence, Expectations, and Intake Review
Oral HA appears in supplements positioned for skin hydration and joint comfort. Patients may ask about hyaluronic acid supplements benefits after hearing social media claims or reading reviews. The evidence base is mixed and product-dependent, and the quality of over-the-counter supplements can vary. For clinics, the practical goal is not to “sell” supplements. The goal is to standardize how staff discuss uncertainty, label claims, and safety screening boundaries.
When a patient asks what is hyaluronic acid in a supplement context, it helps to explain that oral HA must be digested and absorbed before any systemic effect is possible. Manufacturers may use different molecular weights or blends with other ingredients. That makes cross-product comparisons hard. If your clinic carries supplements, build a policy for vendor qualification, label review, and adverse event intake documentation. Also ensure staff avoid medical claims, especially for joint disease or inflammatory conditions.
Questions about hyaluronic acid supplements dosage are common. Avoid giving numeric dosing directions unless you are referencing the specific product label and your local scope allows counseling. A safer operational approach is: confirm the patient is using the labeled serving size, screen for pregnancy/lactation and relevant comorbidities per clinic policy, and document the product name and ingredients. If a patient is under specialist care, advise them to coordinate questions with that clinician.
Trust cue: Clinics should use authentic, manufacturer-labeled products with clear lot and expiry details.
Risk Framing and hyaluronic acid side effects Across Use Types
Clinicians and coordinators need a consistent way to explain risks without overstating them. hyaluronic acid side effects depend heavily on route of use. Topical HA is generally well tolerated, but irritation can occur due to preservatives, fragrance, or overly aggressive routines. Oral supplements can cause nonspecific gastrointestinal upset in some people, and blends may include allergens or interacting ingredients. Injectable HA devices carry procedure-related risks that are not comparable to a serum.
In the injectable setting, adverse events may include bruising, swelling, nodules, infection, or vascular compromise. These are serious topics that require clinician training, emergency preparedness, and clear escalation pathways. Clinics should avoid casual language that minimizes these risks. Even when events are uncommon, they are operationally high impact.
Addressing “organ harm” and cancer concerns responsibly
Patients may search phrases like “hyaluronic acid side effects cancer” or worry about liver or kidney effects. In most routine topical use, systemic exposure is limited. For supplements, systemic exposure is possible but varies by formulation and individual factors. Clinics should avoid definitive reassurance when the patient’s question is really about overall risk tolerance and medical history. Instead, document the concern, confirm what product they mean, and encourage coordination with the patient’s treating clinician for complex histories.
- Route first: clarify topical, oral, or injectable exposure.
- Product specifics: capture full name and ingredients.
- Timeline: note start date and symptom onset.
- Severity: document red flags and escalation steps.
- Reportability: follow local adverse event pathways.
Clinic Operations: Verification, Storage, and Recordkeeping
HA-related products often touch multiple clinic teams. Front desk fields questions, nurses support aftercare messaging, and procurement manages receiving and inventory. A shared workflow reduces preventable errors. It also improves consistency when patients switch between topical routines and in-clinic services.
In a wholesale environment, the basics matter: verify the supplier’s licensing requirements, maintain product traceability, and align storage to the IFU. If your clinic relies on US distribution for predictable replenishment, document how backorders or substitutions are handled to avoid last-minute treatment plan changes.
Quick tip: Record lot numbers at receiving and at point of use.
- Supplier qualification: confirm licensing and documentation process.
- Receiving checks: inspect packaging integrity and labeling.
- Traceability: capture lot, expiry, and storage conditions.
- Protocol alignment: map products to staff competencies.
- Consent language: keep risks format-specific and accurate.
- Adverse events: define escalation and reporting steps.
- Audit readiness: retain records per local requirements.
When training staff, it can help to pair internal SOPs with deep-dive reading. Examples include Profhilo Injections, Viscoderm Hydrobooster, and Restylane Skinboosters Vital Enhances Skin Hydration. If your site inventory includes devices like Viscoderm Hydrobooster Product Listing, keep your internal references tied to IFU language rather than marketing summaries.
Trust cue: Reputable suppliers use screened distribution channels and documentation to support product provenance.
Authoritative Sources
- FDA overview of dermal fillers and safety
- American Academy of Dermatology filler basics
- NIH PubChem entry for hyaluronic acid
In day-to-day operations, what is hyaluronic acid matters less than how you control variability. Use route-specific counseling, verify product documentation, and keep records that support traceability. When claims feel vague, defer to the IFU and authoritative references.
This content is for informational purposes only and is not a substitute for professional medical advice.