
Key Takeaways
- Two-layer model: Papillary (superficial) and reticular (deep) dermis differ in structure and function.
- Procedure relevance: Layer depth affects sensation, bleeding risk, and product placement.
- Interface matters: The dermis-hypodermis junction changes by body site and age.
- Documentation: Record intended tissue plane, device, and lot/UDI where applicable.
Overview
Skin anatomy comes up in injections, device-based treatments, wound care, and dermatologic assessments. In daily practice, teams often ask, what are the two layers of the dermis, and how do they behave under needles, cannulas, and energy devices. This page reviews dermis layers, plain-language synonyms, and what each layer contains. It also links structure to practical considerations like hemostasis, sensory response, and tissue handling.
We cover dermis location relative to the epidermis layers and the hypodermis (subcutaneous fat). We also summarize key histology terms, including extracellular matrix (supportive scaffold) and fibroblasts (collagen-producing cells). Throughout, the focus is operational: how to communicate depth, document technique, and align products with labeled use and clinic policy.
MedWholesaleSupplies operates as a business-to-business supplier intended for healthcare professionals, which is relevant when your clinic standardizes documentation and sourcing across services.
What Are The Two Layers Of The Dermis
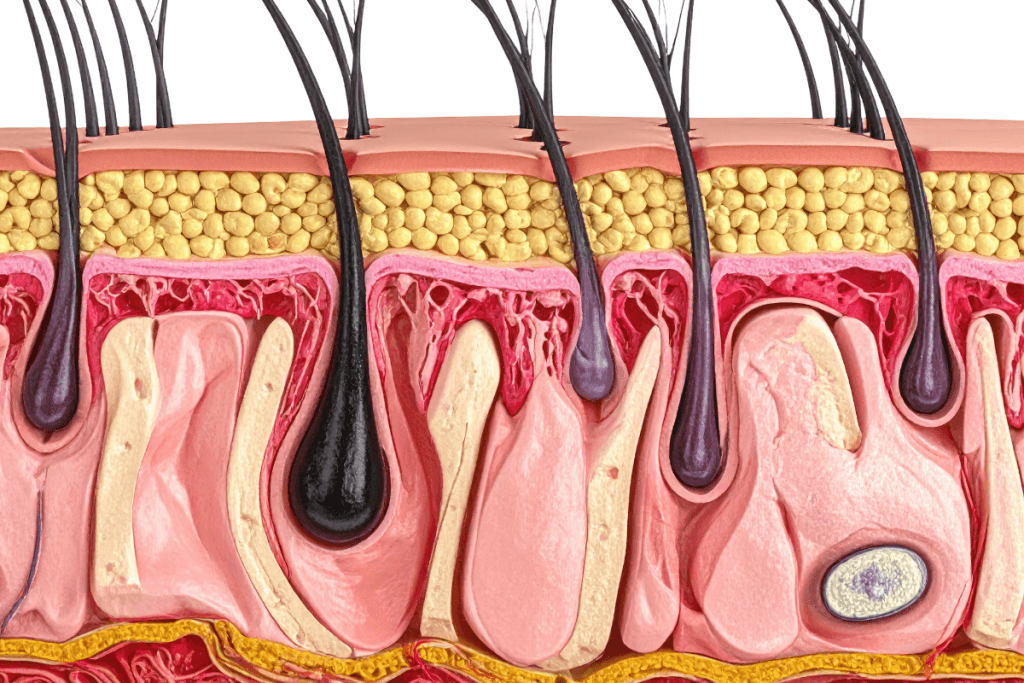
The dermis sits below the epidermis and above the hypodermis. It is connective tissue that provides mechanical strength, elasticity, and a biologically active environment for immune and repair processes. Clinically, it is also a high-information layer: it contains many of the structures that drive bleeding, pain, and edema during skin procedures.
The superficial dermis is the papillary layer. The deeper dermis is the reticular layer. These layers are continuous rather than sharply separated, but they have consistent differences in collagen architecture, vascular density, and the way they interface with skin appendages. Understanding that gradient helps teams describe “intradermal,” “superficial dermal,” and “deep dermal” placement with fewer misunderstandings.
Note: Depth language varies across specialties. Pair layer terms with a brief anatomic descriptor (for example, “superficial dermis near the dermal-epidermal junction”).
Core Concepts
Dermis Location Within the Skin
The dermis location is between the epidermis layers and the hypodermis. The epidermis is an avascular barrier with distinct strata (for example, stratum corneum and stratum basale). In contrast, the dermis is vascular and richly innervated, which is why small depth changes can alter bleeding and discomfort.
When clinicians ask what are the two layers of the dermis, they are usually trying to map clinical terms to real tissue planes. “Superficial dermal” commonly corresponds to the papillary dermis. “Deep dermal” corresponds more closely to the reticular dermis. “Subcutaneous” typically indicates hypodermis tissue, although the dermis-hypodermis interface can be interdigitated and irregular by site.
Papillary Layer: Microanatomy and Function
The papillary layer of dermis is the thin, superficial region that interlocks with the epidermis through dermal papillae. Histologically, it is commonly described as areolar connective tissue (a looser collagen arrangement). This architecture supports nutrient diffusion to the avascular epidermis and allows flexibility during shear.
Papillary layer of dermis function includes thermoregulation, immune surveillance, and sensory signaling. Its superficial vascular plexus (network of blood vessels) can make it more reactive to minor trauma. From a plain-language standpoint, it is the “upper dermis” where capillary refill and many inflammatory changes are most visible.
Reticular Layer: Microanatomy and Function
The reticular layer of dermis is thicker and deeper, with more densely packed collagen bundles and elastic fibers. It is commonly described as dense irregular connective tissue, reflecting multidirectional tensile strength. This is one reason the deeper dermis resists deformation and contributes to skin’s “firmness” on palpation.
Reticular layer of dermis function includes structural support, resilience, and hosting larger neurovascular structures. Many adnexal structures extend into this layer, and the deeper vascular plexus contributes to heat exchange and inflammatory response. In procedure planning, the reticular dermis is also where inadvertent deeper placement may change diffusion patterns and tissue response.
What the Dermis Contains and Why It Matters
For day-to-day communication, it helps to answer “what does the dermis contain” in a consistent way. The dermis contains collagen and elastin fibers, fibroblasts, immune cells, blood vessels, lymphatics, and nerve endings. It also supports skin appendages such as hair follicles, sebaceous glands, and sweat glands, depending on body site.
Dermis function can be summarized as barrier support (through mechanical integrity), sensation, thermoregulation, and repair. Clinically, this is why bruising, swelling, or altered sensation after skin procedures often reflect dermal microvascular or neural involvement rather than epidermal change alone.
Hypodermis: Composition and Interface With the Dermis
The hypodermis (subcutaneous layer) sits beneath the dermis and is often considered part of the integument in practical settings. If your team asks “what is the hypodermis composed of,” a useful answer is adipose tissue organized in lobules, loose connective tissue septa, and larger-caliber vessels and nerves. Hypodermis cells are predominantly adipocytes, with supporting stromal and immune cells.
Hypodermis function includes cushioning, insulation, and energy storage. It also acts as a glide plane over deeper fascia. For many injection workflows, “subcutaneous” targets this layer, but the thickness varies widely by anatomic site, BMI, and age. That variability is a common source of inconsistent depth descriptions across staff.
Practical Guidance
In clinical workflows, dermal anatomy matters most when it reduces ambiguity. A shared internal definition of planes supports safer handoffs, clearer charting, and more consistent outcomes across operators. Even when teams agree on the device, they may not agree on the target tissue plane without a short depth statement.
When documenting what are the two layers of the dermis for training or competency checklists, keep it operational. Use “papillary (superficial) dermis” and “reticular (deep) dermis,” then add a one-line description of expected tissue feel and visible response that your clinic considers typical. Always align technique and indications to the product labeling and institutional policy.
- Standardize depth terms: Define superficial dermal, deep dermal, and subcutaneous in your SOP.
- Record the tissue plane: Chart the intended layer plus anatomic site.
- Capture device identifiers: Include lot, UDI, or serial when applicable.
- Use appropriate tools: Match needle or cannula choice to the planned plane.
For example, some clinics use intradermal delivery devices such as Micronjet when they need consistent superficial placement for specific protocols, which can simplify staff training. Others keep fine-gauge options like Fillmed Nanosoft Microneedles available to support controlled, shallow passes where appropriate to labeled use. For deeper soft-tissue approaches, teams may prefer blunt options like a Softfil Cannula to reduce tissue trauma in selected techniques.
Tip: When onboarding staff, pair a brief anatomy review with photo-based site mapping from your own clinic templates.
Compare & Related Topics
Many “dermis layers and functions” discussions become clearer when contrasted with adjacent layers. The epidermis is primarily barrier and renewal, with named strata that vary by body site (palms and soles have a prominent stratum lucidum). The dermis is supportive and reactive, with vasculature and nerves. The hypodermis is mainly adipose and septal connective tissue, acting as padding and a glide plane.
In practice, the question what are the two layers of the dermis often comes up during injection planning, because clinical endpoints can shift when placement crosses from superficial to deep dermis, or into the subcutis. These same concepts apply beyond aesthetics. For musculoskeletal injection workflows, skin and subcutaneous thickness over a target joint can influence approach and patient comfort. If your team wants adjacent procedural context, see Supartz Vs Euflexxa for how clinics compare intra-articular options, Types Of Gel Injections for a technique overview, and Hymovis Injection for procedure-adjacent considerations.
| Layer | Plain-language description | Typical contents | Why clinics care |
|---|---|---|---|
| Papillary dermis | Upper dermis | Fine collagen, superficial capillaries, sensory endings | Surface reactivity, erythema, superficial bleeding patterns |
| Reticular dermis | Deeper, thicker dermis | Dense collagen bundles, deeper plexus, adnexal support | Tensile strength, deeper pain signals, support for appendages |
| Hypodermis | Subcutaneous fat layer | Adipose lobules, septa, larger vessels and nerves | Glide plane, variable thickness, common injection target |
Clinic Ordering and Compliance Notes
Many clinics tie anatomy education to purchasing controls, because device choice can imply an intended tissue plane. If you stock multiple tools for superficial and deeper approaches, align them to written indications, training sign-off, and standardized charting language. Ordering through professional channels should support traceability, especially for regulated devices and prescription products.
When teams discuss what are the two layers of the dermis during onboarding, it is a good moment to confirm how your clinic verifies product provenance and documentation requirements. MedWholesaleSupplies sources brand-name medical products through verified distribution pathways intended for professional use, which can support internal compliance reviews.
Ordering on MedWholesaleSupplies is restricted to licensed clinics and qualified healthcare professionals. For clinics that pair procedures with adjunctive skin support, the Clinical Skincare category can be used as a reference hub when building formulary-aligned protocols. Some practices also keep clinic-use consumables such as Jalupro Biocellulose Face Masks available for post-procedure workflows, where consistent documentation and infection-control handling are part of routine operations.
Authoritative Sources
For deeper review of skin structure and dermis histology, these references provide standard terminology and context:
- NCBI Bookshelf (StatPearls): Anatomy, Skin (Integument)
- NCBI Bookshelf (StatPearls): Histology, Dermis
- OpenStax Anatomy & Physiology: Layers of the Skin
Clear layer language reduces errors in training, documentation, and product selection. Use consistent terms, confirm planes during competency checks, and defer to labeling and clinic policy when technique questions arise.
This content is for informational purposes only and is not a substitute for professional medical advice.



